Degenerative Meniscus Tears
If you’re over 45 and experiencing knee pain, stiffness, or swelling, you may have a degenerative meniscus tear. Unlike traumatic meniscus tears that occur from a specific injury during sports or activity, degenerative tears develop gradually as the meniscus tissue weakens with age and use. These tears are extremely common — imaging studies show meniscal tears in approximately 35% of people over age 50, and many of these tears are asymptomatic.
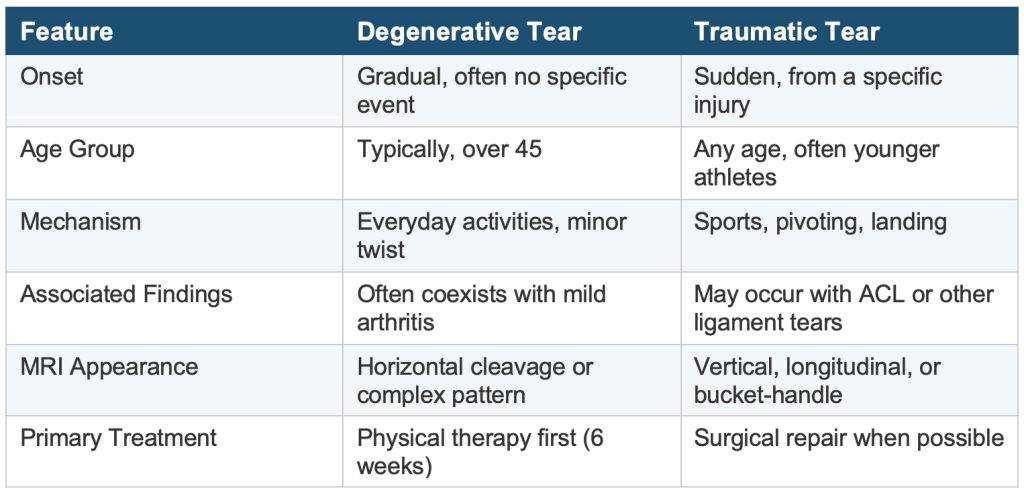
Understanding the difference between a degenerative meniscus tear and a traumatic tear is critical because the treatment approach is fundamentally different. Dr. Ronak Patel, serving patients across Chicagoland, takes an evidence-based, patient-centered approach to ensure you receive the right treatment for your specific situation.
The meniscus changes with age. Over time, the collagen fibers that make up the meniscus become less organized, and the tissue becomes more brittle and prone to tearing with minimal or no trauma. Common factors that contribute to degenerative tears include:
- Age-related tissue changes (most significant after age 45)
- Cumulative wear from years of activity
- Early or mild osteoarthritis
- Occupational factors such as repetitive kneeling, squatting, or heavy lifting
The 2024 EU-US Meniscus Rehabilitation Consensus confirmed that work-related lifting and carrying (over 10 pounds), kneeling, deep squatting, and high-volume climbing are associated with increased risk of meniscus injury (Grade A evidence).
This distinction matters enormously for treatment:
The evidence is now clear and consistent: for most degenerative meniscus tears, physical therapy produces outcomes equivalent to surgery. The landmark ESCAPE trial, with 5-year follow-up published in JAMA Network Open (2022), demonstrated that exercise-based physical therapy was non-inferior to arthroscopic partial meniscectomy for patient-reported knee function. The authors concluded that physical therapy should be the preferred initial treatment for degenerative meniscal tears.
A 2025 systematic review and meta-analysis with 5-year follow-up across six randomized controlled trials (1,157 patients) confirmed these findings, showing no significant difference in knee function scores, activity levels, or meniscal evaluation scores between surgery and non-operative treatment.
Dr. Patel’s approach aligns with these guidelines. For patients with degenerative meniscus tears, he recommends an initial course of structured physical therapy lasting at least 6 weeks, which typically includes:
- Progressive quadriceps, hamstring, and hip strengthening exercises
- Neuromuscular and balance training
- Manual therapy and joint mobilization
- Activity modification and patient education
Many patients experience significant improvement with this approach and do not require surgery.
While physical therapy is the preferred first-line treatment, surgery may be appropriate in specific circumstances:
- True mechanical symptoms: A locked knee (inability to fully straighten) caused by a displaced meniscus fragment is generally an indication for surgery.
- Failure of conservative treatment: Patients who complete a thorough course of physical therapy (~6 weeks) without meaningful improvement may benefit from arthroscopic evaluation.
- Co-existing conditions: Some patients have a combination of a degenerative tear and a repairable component that may warrant surgical attention.
When surgery is indicated for a degenerative tear, a partial meniscectomy (removing only the unstable, damaged portion) is the most common procedure. The goal is to remove as little tissue as possible to relieve symptoms while preserving as much meniscus as feasible.
Degenerative meniscus tears and knee osteoarthritis frequently coexist, and this overlap complicates treatment decisions. An MRI showing a meniscus tear does not necessarily mean the tear is causing your symptoms — the underlying arthritis may be the primary pain generator. This is why a thorough clinical evaluation, not just imaging, is essential.
Research has shown that meniscectomy may worsen cartilage degeneration over time. One study found a five-fold higher risk of total knee replacement after surgery compared to physical therapy, though other studies have shown no significant difference. Dr. Patel carefully weighs these factors when making treatment recommendations.
In addition to physical therapy, Dr. Patel may recommend adjunctive treatments to manage symptoms:
- Platelet-Rich Plasma (PRP) Injections: Concentrated growth factors from your own blood may help reduce inflammation and support tissue healing.
- Bone Marrow Aspirate Concentrate: Contains mesenchymal stem cells that may support cartilage health.
- Laser Therapy: May help reduce pain and inflammation as a complement to physical therapy.
- Anti-inflammatory medications: Short-term use of NSAIDs can help manage acute flare-ups.
Dr. Patel takes a conservative-first, evidence-based approach to degenerative meniscus tears. He will not recommend surgery unless the clinical picture clearly supports it. His philosophy prioritizes:
- Thorough evaluation to distinguish meniscus symptoms from arthritis symptoms
- Structured physical therapy as a first-line treatment
- Meniscus preservation when surgery is indicated
- Biologic treatments to support tissue health
Experiencing knee pain and wondering if you have a meniscus tear? Schedule a consultation with Dr. Ronak Patel
References
- Noorduyn JCA, et al. Effect of Physical Therapy vs Arthroscopic Partial Meniscectomy in People With Degenerative Meniscal Tears: Five-Year Follow-up of the
- ESCAPE Randomized Clinical Trial. JAMA Network Open. 2022;5(7):e2220394.
- Arthroscopic Surgery vs. Physical Therapy for Degenerative Meniscal Tears. Am Fam Physician. 2024;110(4):421-422.
- Prill R, et al. The Formal EU-US Meniscus Rehabilitation 2024 Consensus: An ESSKA-AOSSM-AASPT Initiative. JOSPT Open. 2025;3(3).
- Katz JN, et al. Surgery versus Physical Therapy for a Meniscal Tear and Osteoarthritis. N Engl J Med. 2013;368(18):1675-1684.
At a Glance
Ronak M. Patel M.D.
- Double Board-Certified, Fellowship-Trained Orthopaedic Surgeon
- Team physician to the Chicago Hounds (MLR) and past team physician to the Cavaliers (NBA), Browns (NFL) and Guardians (MLB)
- Published over 50 publications and 10 book chapters
- Learn more